
In the past decade Malawi has made significant progress in key health programs, improving treatment coverage, prevention efforts, and overall population-level outcomes. The country has expanded HIV treatment, strengthened disease surveillance, and pushed forward lifesaving interventions in maternal and child health. Beneath these achievements, however, lies a precarious truth. Malawi’s health system is standing on the edge of a steep cliff, supported by a financial structure that could collapse with a single shift in donor priorities.
At the center of this fragility is an uncomfortable reality. More than half of the national health budget is funded by external partners. In the 2024 and 2025 fiscal cycle alone, donors contributed 56 percent of all health sector resources. Nowhere is this dependence more visible than in the HIV response. An extraordinary 97 percent of HIV and AIDS financing comes from global funders rather than domestic sources. These numbers show remarkable generosity from the international community, but they also reveal a system that cannot sustain itself if the flow of external support slows down.
This vulnerability became painfully clear in early 2025 when a USAID funding freeze rippled through the system. The impact was immediate. Facilities that were already struggling with staffing shortages, weak diagnostics, and low service readiness saw conditions deteriorate even further. Malawi’s overall readiness score, which once hovered around 60 percent, dropped to below 50 percent. The shock exposed how thin the margin for stability really is.
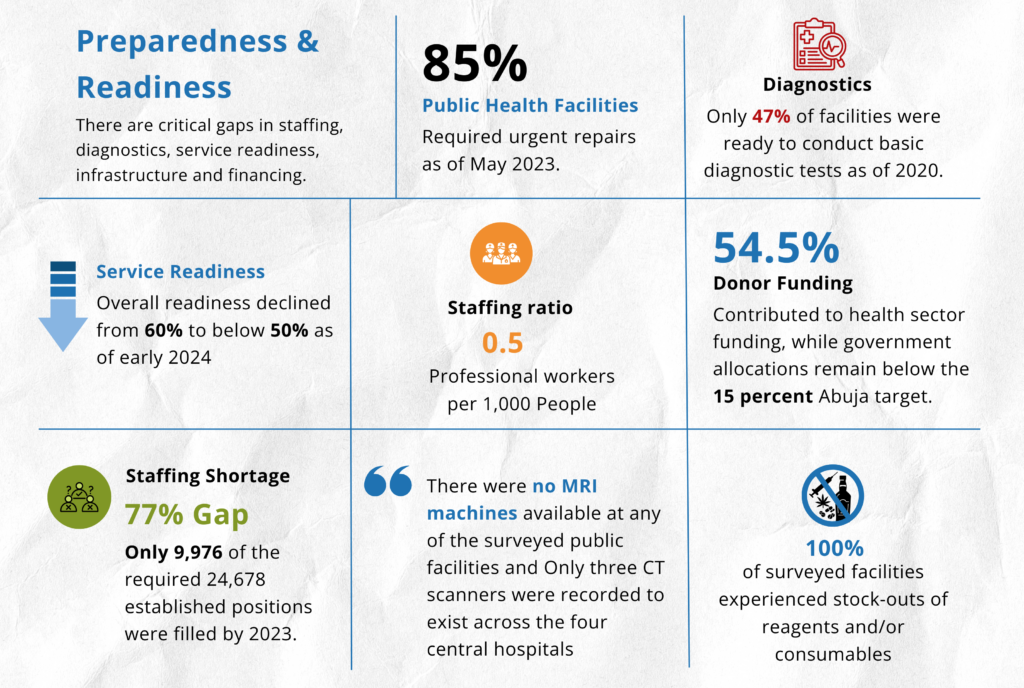
The challenge becomes even more concerning when held against domestic financing patterns. Although the government increased its health allocation to 12.2 percent of the national budget for 2024 and 2025, this level still falls short of the 15 percent Abuja target that Malawi committed to more than two decades ago. The gap may seem small, but in practical terms it means fewer health workers, fewer functioning medical devices, fewer emergency reserves, and fewer chances to build a resilient foundation that can survive global funding shifts.
Despite these warning signs, Malawi’s health landscape continues to be shaped by donor-driven vertical programs. These programs have been undeniably successful in areas like HIV treatment scale-up, malaria prevention, and TB control. The issue is not the programs themselves, but the fragmentation they create. When large portions of the system are designed around disease-specific priorities rather than integrated national planning, the result is a patchwork of pockets of excellence surrounded by areas of chronic neglect. One crisis in a major funding stream can send shockwaves across services that depend on stable, predictable financing.
Malawi is not alone in this. Many low and middle income countries face similar patterns of dependency and structural imbalance. What makes Malawi’s situation urgent is the degree of reliance combined with declining system readiness, low staffing ratios, infrastructure gaps, and a widening financing shortfall. The data tells a clear story. The health system has been running on borrowed stability, surviving through goodwill rather than sustainable investment.
The question now is how long this model can hold. The world has changed. Funding landscapes are becoming more competitive. Donor priorities continue to shift. Economic shocks and emergencies are reshaping global health financing. Malawi’s health system will need stronger domestic investment and more unified planning to avoid the risk of being pushed over the precipice.
Until then, the country remains only one donor check away from a crisis that has been years in the making.